Dr Kirrilly Thompson and her research team found that Addiction Medicine is a deeply rewarding specialisation, but we need greater visibility and clinical exposure if we want to grow the workforce
“One of medicine’s best kept secrets?” What draws doctors into addiction medicine
June 2026
Teaser image
When Australians think about medical specialties, they often picture surgery, emergency medicine, psychiatry or paediatrics. Far fewer are aware of addiction medicine, despite alcohol and other drug (AOD) issues touching almost every corner of the health system and community.
Addiction medicine is a specialist field focused on the prevention, assessment and treatment of addiction, including substance use disorders and gambling-related harms. Yet, despite growing need, it remains a relatively small workforce. Recent evidence to a parliamentary inquiry noted there are around 240 Fellows of the Chapter of Addiction Medicine. Including colleagues in Aotearoa New Zealand, those not currently in active clinical practice and approximately 80 trainees, the broader addiction medicine workforce numbers around 370 clinicians.[1] At a time when substance-related harms continue to impact individuals, families and communities, understanding how to attract and sustain this workforce matters more than ever.
Our newly published research sought to better understand what motivates doctors to specialise in addiction medicine, what concerns they have, and what might encourage more clinicians to enter the field.
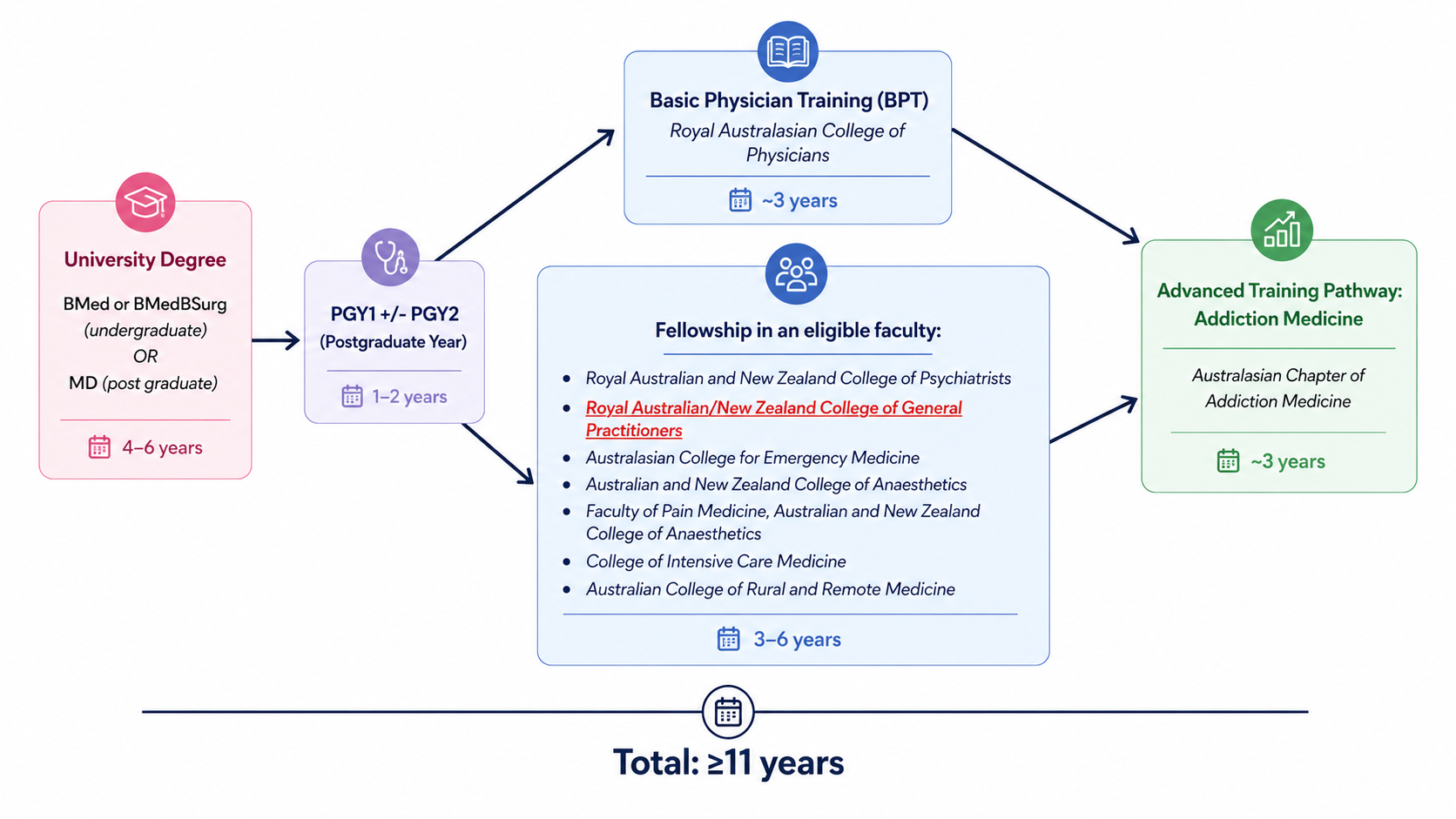
We interviewed 22 Addiction Medicine Fellows and Trainees across Australia and Aotearoa New Zealand. All participants had entered addiction medicine through the General Practice (GP) pathway, the most common route into the specialty. Their reflections offered valuable insight into how experienced GPs come to see addiction medicine not simply as an additional qualification, but as a rewarding career pathway.
Discovering addiction medicine, often by chance
One of the clearest findings from our research was that many doctors discovered addiction medicine accidentally. For some, it happened through a placement, a mentor or an unexpected conversation. Others stumbled across the specialty almost by accident while working in AOD settings.
As one trainee explained:
“I had no idea this existed… when I spoke to someone and they said you can get a fellowship in it, my heart leapt and I was like, ‘Oh my God, that would be amazing because I’ve always wanted to specialise.’”
Another Fellow recalled:
“Literally what happened is I went to a dinner party… and someone suggested that I might consider coming to work for them.”
For a specialty that addresses one of Australia’s major health challenges, the finding that many doctors encounter addiction medicine serendipitously raises important questions. If clinicians do not know the specialty exists, how can they imagine a future within it? As one trainee put it:
“No one hears about it and you can’t be it if you can’t see it.”
Participants therefore repeatedly reflected on the need for greater visibility of addiction medicine, particularly during medical school, junior doctor training and GP registrar years.
Meaningful work and real impact
Participants described addiction medicine as intellectually interesting, highly relational and deeply meaningful. Many spoke about the privilege of walking alongside people experiencing significant challenges and seeing meaningful improvements in health and wellbeing over time. One Fellow reflected:
“Working with alcohol and drug patients, they generally get well… They’ve made some real changes.”
Another described addiction medicine as one of the few areas of medicine where clinicians can make profound differences in people’s lives:
“Of all the areas of medicine, I think it’s the one that we can actually make one of the biggest difference to people’s lives.”
Importantly, addiction medicine was often described as aligning closely with participants’ values. Participants spoke about advocacy, reducing stigma and supporting people who may have experienced significant marginalisation. For some, specialising in addiction medicine was not simply about career progression, but also about helping legitimise a field that has historically been overlooked.
Participants also valued the diversity of the work. They described opportunities spanning inpatient care, outpatient settings, withdrawal management, consultation liaison, public health, service development, education and leadership. Many appreciated the flexibility and variety compared with their previous GP roles.
Balancing rewards and trade-offs
While participants overwhelmingly described addiction medicine positively, they also reflected candidly on concerns. Because all participants had entered through the GP pathway, many worried about losing some of their generalist skills. Others described the financial realities of advanced training, including reduced income during training years and the challenge of balancing study with family responsibilities. However, most felt the benefits outweighed the sacrifices.
Several participants highlighted strong collegial support, mentorship and a workplace culture that felt collaborative and meaningful. Work-life balance was also seen as an unexpected benefit, particularly compared with other specialist pathways.
As one trainee described it:
“This is probably, if not the most work-life friendly job as a specialty.”
What happens next?
Our findings suggest there are practical opportunities to strengthen the addiction medicine workforce.
Increasing visibility of the specialty appears especially important. Participants consistently highlighted the value of clinical placements, role models and early exposure in helping clinicians understand what addiction medicine actually involves across a variety of settings.
Perhaps the clearest message from this study is that addiction medicine should no longer remain one of medicine’s “best kept secrets”. Many participants described a career shaped by meaningful patient relationships, strong collegial support and the opportunity to make a tangible difference in people’s lives. Yet many had discovered the specialty only by chance.
As demand for addiction expertise continues to grow, ensuring clinicians can see, experience and imagine a future in addiction medicine will become increasingly important.
Acknowledgements
We are grateful to AChAM’s Member Engagement and Support department for assistance with recruitment and to the Fellows and Trainees who generously shared their opinions and experiences with us.
Further reading
Tawfic, Y., Bartram, A., Bowden, J., Dunlop, A. and Thompson, K. (2026). “Probably one of medicine’s best kept secrets”: preliminary qualitative insights into motivations and concerns regarding addiction medicine specialisation in Australasia. BMC Medical Education. Available at: https://link.springer.com/article/10.1186/s12909-026-09480-5