Changing markets for opioids have implications for responding to the risk of overdose, writes Prof Paul Dietze
Naloxone dosing in opioid overdose response: getting the balance right
June 2025
Teaser image

Opioid overdose is a significant public health issue, driving the majority of drug-related deaths worldwide. Many opioid overdoses are reversable through airway management and the use of naloxone, an opioid antagonist drug that quickly and efficiently reverses the effects of opioid drugs, with few other effects. In many countries naloxone is available for use by emergency medical personnel (e.g., emergency department staff, paramedics), and is increasingly becoming available to other first responders (e.g. police) and broader members of the community who may witness opioid overdoses, through so-called take-home naloxone programs.
Naloxone can be administered in a variety of ways, typically through intravenous or intramuscular injection or through a nasal spray. A range of naloxone formulations are available in Australia, including ampoules, and pre-filled syringes such as Prenoxad® and nasal sprays such as Nyxoid® (pictured below in that order).
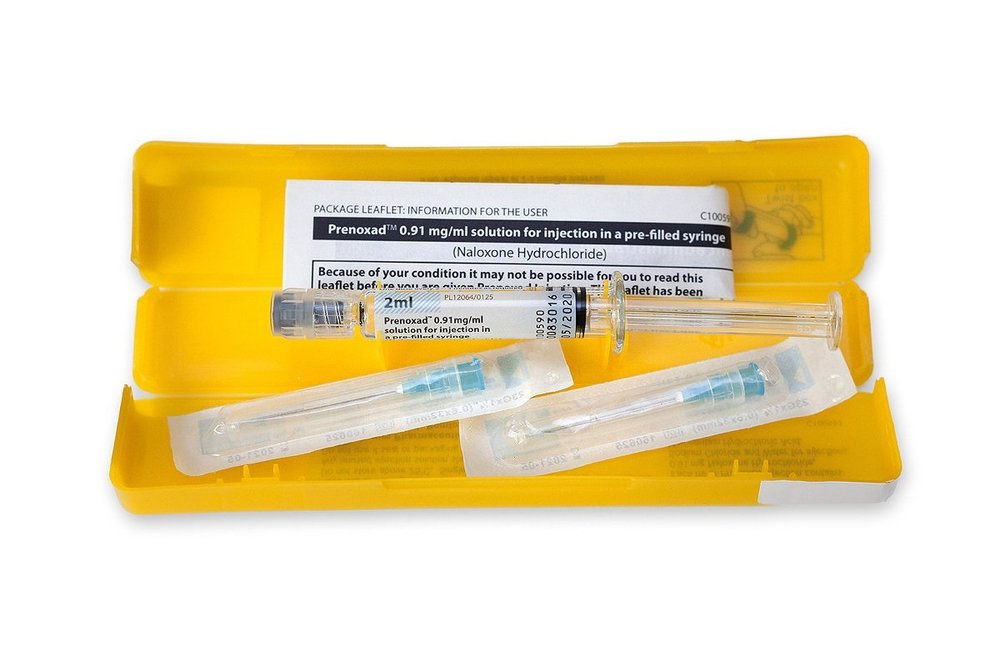
All of these formulations have been devised to provide timely opioid reversal, based on how naloxone is absorbed by the body.
In general, of the three main routes of naloxone administration used, the onset of action is quickest for intravenous administration, followed by the intramuscular and intranasal routes.
These different rates of onset of naloxone action mean that different doses are typically used in opioid overdose response, with defined doses of 0.04 mg and 0.4 mg typically used for intravenous and intramuscular injection respectively and higher doses of 1.26-10 mg used in intranasal sprays.
This variation has important implications for take-home naloxone programs in particular, as capacity for medical monitoring may be limited. The 2014 guidance from the World Health Organization (WHO) suggested that initial doses of 0.4-2 mg should be administered with additional doses as needed until full recovery has been achieved. Importantly, these guidelines pre-date the availability of concentrated fit-for-purpose intranasal naloxone preparations and so recommendations related to intranasal administration of naloxone were more limited.
Changing markets for opioid drugs, both in terms of the drugs available and their potency, have implications for how to best respond to the possibility of opioid overdose.
In a recent commentary, Strang et al. highlighted some of the reasons why higher doses of naloxone may be needed to reverse effects of potent synthetic opioids like fentanyl and nitazenes that relate not only to the typical opioid overdose symptoms (e.g., respiratory depression) that are produced by these drugs but different effects such as muscle rigidity.
Indeed, high-dose (typically intranasal) formulations of naloxone have been developed for use in response to overdoses involving potent synthetic opioids, presumably as a means of ensuring adequate antagonism response. However, Strang et al. point out that these high doses run the risk of over-antagonism that can lead to opioid withdrawal and other unpleasant side effects. Over-antagonism has the potential to reduce the effectiveness of take-home naloxone programs as people may avoid the use of naloxone when their experiences have been negative. Further, previous work has shown that what amounts to very low doses of naloxone can reverse opioid overdoses, and a recent review suggests that relatively normal naloxone doses were sufficient to reverse nitazene overdoses, meaning that standard doses of naloxone may be sufficient for the vast majority of overdose cases.

In medical settings, titration with escalating naloxone doses is recommended in responding to opioid overdose. However, in settings involving take-home naloxone, current formulations may make such careful titration and monitoring difficult.
The 2014 WHO guidelines outline the typical recommended principle of naloxone administration in cases of opioid overdose – to commence with airway management and an initial naloxone dose (as available) with ongoing airway management and additional naloxone doses every two to three minutes as required (until the person regains consciousness or maintains effective respiration).
This principle is consistent with product information provided for the two mains forms of naloxone supplied under the Australian Take-Home Naloxone Program and provides for some degree of dose titration, also aligning with practices described in relation to opioid overdose responses.
Nevertheless, titration may be more difficult with the intranasal formulations currently available, meaning that it is important to ensure that multiple forms of naloxone are available to allow for consumer choice as more experienced responders may prefer intramuscular naloxone to intranasal naloxone when responding to opioid overdose.
In the end, finding the right dose of naloxone for administration in cases of opioid overdoses is an ‘empirical’ question, determined by the opioid involved and the setting in which their consumption occurs as well as the setting in which response is effected. Australia is fortunate to have a substantial subsidised take home naloxone program that allows for wide availability of different naloxone formulations that supports consumer choice.
As it stands doses routinely available under the program are consistent with recommendations made by recent reviews, and current guidance from the WHO (that is under review), but ongoing monitoring of illicit opioid markets is essential to ensuring that Australia’s opioid overdose response remains fit-for-purpose.
Image sources: nuaa.org.au, nyxoid.com.au