
Australia’s alcohol policy ranking does not match its alcohol consumption ranking: what’s going on?
November 2014

Australia ranks first in terms of the number of alcohol policies it has and its enforcement of those policies, yet alcohol consumption exceeds that of other countries. NDARC researchers explore why this may be the case.
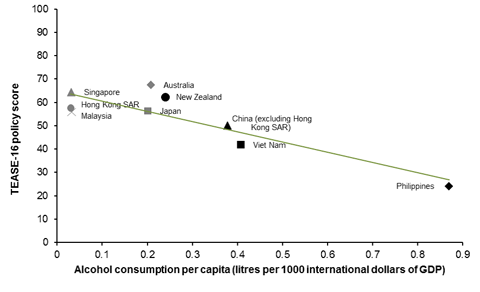
New findings published in the WHO bulletin show that, among nine countries in the western pacific, Australia ranks first in terms of the number of alcohol policies it has and its enforcement of those policies, but is mid-field in terms of its rate of alcohol consumption, even taking into account population sizes and relative national wealth (GDP). This either calls into question the effectiveness of alcohol policies, or says that policies alone don’t entirely determine the extent of drinking in a country: in scientific parlance, it could mean that alcohol policies are a necessary but insufficient explanation of alcohol consumption rates.
This research, conducted by the National Drug and Alcohol Research Centre (NDARC) and the Hunter Medical Research Institute, does not support the possibility that alcohol policies are ineffective. A graph of the nine western pacific countries shows a clear linear relationship between the strength of alcohol policies plus their enforcement (measured using a new 16-item scale developed by the researchers called the Toolkit for Evaluating Alcohol policy Stringency and Enforcement or TEASE-16) and per capita alcohol consumption. Specifically stronger policies are associated with lower per capita alcohol consumption.
If alcohol policies are effective in limiting per capita alcohol consumption in a country, then the only other explanation for these results is that there is some other factor, or group of factors, mediating the relationship between policies and per capita consumption. These could include cultural norms, religious practices and even biological or genetic factors that are not yet understood. This seems the most likely explanation and is consistent with existing research that has shown significant differences in rates of risky drinking, alcohol-related crime and alcohol-related traffic crashes even in communities that are under exactly the same legislative framework with NSW.
This research has three key policy implications. First, matching policies to their specific intended impact is important: these data show a benefit in terms of per capita alcohol consumption generally, but say nothing about patterns of drinking which is critical in countries like Australia where most risky drinking is associated with weekend binge drinking rather than excessive regular drinking. The policies that impact on average consumption may not be the same policies that impact on binge drinking, as we have highlighted in relation to policies on alcohol price.
Second, there is ample room to further strengthen alcohol policies internationally. Even Australia, as the highest ranked country, only scored 67.5 out of 100. Compared to other countries, Australia was relatively weak on alcohol advertising and pricing policy.
Third, it is unlikely that policy initiatives alone will be optimal in reducing risky drinking. Our methodologically rigorous RCT evidence has highlighted that complementary community-action is not simply a feel-good idea: it achieved a statistically significant 20% reduction in average weekly alcohol consumption in experimental, relative to control, communities. Although this might seem a modest benefit at face value, a 10% reduction in average consumption in a community has been estimated to equate to 25% fewer individuals engaging in heavy drinking (≥24 standard drinks/week).
Last week’s AMA National Alcohol Summit in Canberra put the focus on Australia’s national alcohol policies and they are under further examination in the current competition policy review being chaired by Professor Ian Harper. Whatever the outcome of those deliberations, minimising alcohol harm in Australia is most likely to be achieved by ensuring a clear line of sight from the policy to its intended outcome, strengthening existing policies, especially in relation to advertising and price in Australia, and funding community-level activity that has rigorous evidence for its effectiveness.
TEASE-16 was developed and evaluated by Dr Natacha Carragher and Professor Anthony Shakeshaft of the National Drug and Alcohol Research Centre and Dr Joshua Byrnes and Professor Christopher Doran of the Hunter Medical Research Institute.



